If your veterinarian has told you that your dog or cat has a mast cell tumor, you are likely feeling a mix of worry and confusion. These tumors are among the most common skin tumors found in pets, particularly in dogs, and while a diagnosis can be frightening, understanding what mast cell tumors are and how they are treated can help you make informed decisions alongside your veterinary team.
What Are Mast Cells?
Mast cells are a normal part of the immune system. They are found throughout the body in connective tissue and near blood vessels, and they play a role in allergic reactions, wound healing, and defense against parasites. When mast cells multiply in an uncontrolled way, they form a tumor.
These tumors contain granules filled with substances like histamine and heparin. When mast cells are disturbed or the tumor is manipulated, those granules can release their contents into the surrounding tissue and bloodstream. This is called degranulation, and it can cause local irritation or, in more serious cases, systemic effects such as stomach ulcers or drops in blood pressure.
Mast Cell Tumors in Dogs:
How Common Are They?
Mast cell tumors are the most frequently diagnosed malignant skin tumor in dogs, accounting for roughly 20 percent of all skin tumors. They can appear in dogs of any age, though they are more common in middle aged and older dogs. Certain breeds are at higher risk, including:
Boxers
Bulldogs (English and French)
Boston Terriers
Pugs
Labrador Retrievers
Golden Retrievers
Shar Peis
Beagles
What Do They Look Like?
Mast cell tumors are sometimes called “the great pretenders” because they can look like almost anything. They may appear as:
A raised, smooth lump under the skin
A firm nodule at the skin surface
A soft, fatty feeling mass
A red, ulcerated, or irritated sore
Some tumors stay small for years while others grow rapidly. Because appearance alone cannot tell you whether a lump is a mast cell tumor, any new or changing growth on your dog should be evaluated by a veterinarian.
Important: Never squeeze, massage, or repeatedly touch a suspected mast cell tumor. Doing so can trigger degranulation and worsen symptoms.
Grading and Staging
Once a mast cell tumor is diagnosed, your veterinarian will work to understand how aggressive it is. This involves two key processes: grading and staging.
Grading refers to how the tumor cells look under the microscope. The most widely used system divides tumors into three grades:
Grade 1 (low grade): Well organized cells that tend to behave less aggressively
Grade 2 (intermediate grade): More variable behavior; can be difficult to predict
Grade 3 (high grade): Poorly organized cells associated with more aggressive behavior and a greater chance of spreading
Staging determines whether the cancer has spread beyond the original site. This may involve lymph node sampling, blood work, imaging such as ultrasound, and sometimes a bone marrow biopsy.
Treatment Options
Treatment depends on the tumor grade, location, and whether it has spread. Your veterinarian or veterinary oncologist will help you choose the right path for your dog.
Surgery is the primary treatment for most mast cell tumors. The goal is to remove the tumor along with a margin of healthy tissue around it to reduce the chance of regrowth. For tumors in easy to access locations, surgery alone may be curative.
Radiation therapy is often used when surgery cannot remove all the tumor tissue, particularly for tumors in challenging locations like the face, paws, or groin.
Chemotherapy may be recommended for high grade tumors, cases where the disease has spread, or when surgery and radiation are not enough on their own.
Targeted therapy with drugs such as toceranib phosphate (Palladia) or masitinib targets specific proteins that help some mast cell tumors grow. These are oral medications that some dogs tolerate well.
Prognosis
The outlook for dogs with mast cell tumors is highly variable. Low grade tumors that are completely removed surgically often have excellent long term outcomes. High grade tumors or those that have spread are more challenging to treat, though many dogs still enjoy a good quality of life with the right management. Your veterinarian can help set realistic expectations based on your individual dog’s situation.
Mast Cell Tumors in Cats:
Are They the Same as in Dogs?
Mast cell tumors in cats are less common than in dogs and they behave somewhat differently. In cats, these tumors are the second most common skin tumor overall, but they also occur in the spleen and intestines, which is less typical in dogs.
Skin Mast Cell Tumors in Cats
Cutaneous (skin) mast cell tumors in cats most often appear as small, firm, raised lumps. They are frequently found on the head and neck. Siamese cats appear to be predisposed and may develop multiple small skin tumors, often referred to as histiocytic mast cell tumors, which in young Siamese cats tend to resolve on their own over time.
Most cutaneous mast cell tumors in cats are considered low grade and behave less aggressively than their canine counterparts. Surgical removal is usually the recommended treatment and can be curative.
Splenic Mast Cell Tumors in Cats
The spleen is the most common internal site for mast cell disease in cats. Cats with splenic mast cell tumors may show signs such as:
Weight loss and decreased appetite
Vomiting or diarrhea
Lethargy
A palpable mass in the abdomen
Surgical removal of the spleen (a procedure called a splenectomy) is the standard treatment and often leads to significant improvement in quality of life. Some cats live for a year or more after surgery, particularly when the disease has not spread widely.
Intestinal Mast Cell Tumors in Cats
Intestinal mast cell tumors are less common and tend to be more aggressive. They can cause signs similar to other gastrointestinal diseases, making diagnosis more challenging. Treatment typically involves surgery and sometimes chemotherapy, though the prognosis is generally more guarded than for the splenic form.
How Is a Mast Cell Tumor Diagnosed?
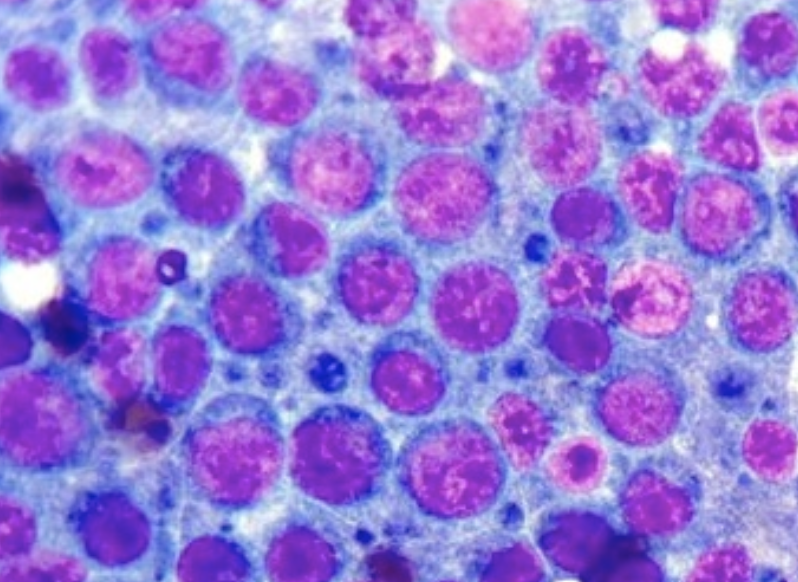
The most common first step in diagnosing a mast cell tumor is a fine needle aspirate. Your veterinarian inserts a small needle into the lump and collects a sample of cells, which are then examined under a microscope. This procedure is quick, minimally invasive, and often done without sedation.
Because mast cells have a distinctive appearance and contain easily visible granules, they are often identifiable on a simple aspirate. However, a biopsy (removal of a piece of tissue for histopathology) is needed to grade the tumor and assess whether the margins are clear after surgery.
Living With a Pet Who Has Had a Mast Cell Tumor
Monitoring for Recurrence
After treatment, regular follow up appointments are essential. Your veterinarian will check the surgical site for signs of regrowth and look for any new lumps. You should also perform regular at home checks and report any new growths promptly.
Most recurrences happen within the first year after surgery. The longer your pet goes without a recurrence, the more encouraging the outlook.
Managing Symptoms Related to Histamine Release
In some cases, especially with larger or more aggressive tumors, your veterinarian may recommend antihistamines such as diphenhydramine or famotidine (an antacid) to help protect the stomach lining from excess histamine. These medications can reduce nausea, vomiting, and stomach ulcer formation.
Quality of Life
Many pets with mast cell tumors go on to live comfortable, happy lives after treatment. With attentive home care, regular veterinary monitoring, and open communication with your veterinary team, you can help your pet maintain a good quality of life throughout their treatment and beyond.
Reminder: Never stop or change your pet’s medications without consulting your veterinarian first. Some treatments require careful tapering or monitoring.
When to Contact Your Veterinarian
You should contact your veterinarian promptly if you notice any of the following:
A new lump or bump anywhere on your pet’s body
A previously diagnosed lump that has changed in size, shape, or texture
Redness, swelling, or oozing around a known tumor site
Vomiting, decreased appetite, or unusual lethargy
Signs of allergic reaction such as facial swelling, hives, or sudden weakness
Questions to Ask Your Veterinary Team
Being prepared for appointments can help you get the most out of your time with the veterinary team. Consider asking:
What grade is this tumor, and what does that mean for my pet?
Has it spread to any lymph nodes or other organs?
What are all the treatment options, and what are the pros and cons of each?
What is the expected recovery time after surgery?
How often should my pet be rechecked, and what should I watch for at home?
Are there any clinical trials that might be appropriate?
What can I do to keep my pet comfortable during treatment?
Final Thoughts
Receiving a mast cell tumor diagnosis for your pet is stressful, but it is far from hopeless. These tumors are well studied, and veterinary medicine has made significant advances in understanding and treating them. Many dogs and cats go on to enjoy long, comfortable lives after diagnosis and treatment.
The most important thing you can do is work closely with your veterinary team, attend all recommended follow up appointments, and stay observant of any changes in your pet. You know your animal better than anyone, and your attentiveness at home is a critical part of their care.
With the right information and support, you can be a strong advocate for your pet every step of the way.
This article is intended for general educational purposes only and does not replace professional veterinary advice. Always consult a licensed veterinarian for guidance specific to your pet.
Understanding oral, digital, and ocular melanomas in your dog
What Is Canine Melanoma?
Melanoma is a type of cancer that arises from melanocytes, the specialized cells responsible for producing melanin, the pigment that gives skin, fur, and eyes their color. In dogs, melanoma is one of the most commonly diagnosed cancers, and it behaves very differently depending on where in the body it develops.
Unlike in humans, where melanoma is most often linked to sun exposure and found on the skin, canine melanoma most frequently develops in the mouth, on the toes, and in or around the eyes. Each location carries its own set of characteristics, risks, and treatment approaches. Understanding the differences can help you recognize potential warning signs early and give your dog the best possible chance for a positive outcome.
This guide is designed to walk you through the three primary forms of canine melanoma: oral (mouth), digital (toes and nail beds), and ocular (eyes). It covers what to look for, what to expect from diagnosis and treatment, and how to support your dog through every stage of the journey.
Why Early Detection Matters Many forms of canine melanoma are aggressive tumors that can spread to lymph nodes, lungs, and other organs. The sooner a melanoma is identified and treated, the greater the likelihood that treatment will be successful. Regular checkups and an attentive eye at home can make a real difference in your dog’s outcome.
Oral Melanoma
Overview
Oral melanoma is the most common form of melanoma diagnosed in dogs. It accounts for roughly 30 to 40 percent of all oral tumors in canines, making it the most frequently seen oral cancer in the species. Oral melanomas are almost always considered malignant, meaning they have a strong tendency to invade surrounding tissue and spread, or metastasize, to other parts of the body.
These tumors typically originate on the gums (gingiva), the palate, the tongue, or the lips. They can appear pigmented (dark brown or black) or, in some cases, amelanotic (lacking visible pigment), which makes them appear pink or red and can cause them to be mistaken for less serious conditions.
Who Is at Risk?
Oral melanoma is more frequently diagnosed in older dogs, with the average age at diagnosis being around 11 years. Certain breeds appear to have a higher predisposition, including:
Cocker Spaniels
Scottish Terriers
Golden Retrievers
Poodles
Chow Chows
Doberman Pinschers
Male dogs appear to develop oral melanoma more often than females, though the reason for this disparity is not fully understood. Dogs with heavily pigmented oral mucosa (the tissue lining the mouth) are generally considered to be at greater risk.
Signs and Symptoms
The signs of oral melanoma can range from subtle to quite noticeable. Pet owners who regularly inspect their dog’s mouth may catch early changes, while others might first notice behavioral or functional changes. Common signs include:
Category
Details
Visible mass
A lump, nodule, or ulcerated area on the gums, tongue, palate, or lips; may be dark, pink, or red
Drooling
Excessive or unusual drooling, sometimes tinged with blood
Bad breath
A sudden or worsening foul odor from the mouth not explained by dental disease alone
Difficulty eating
Dropping food, chewing on one side, or reluctance to eat hard kibble
Facial swelling
Puffiness around the face, jaw, or cheeks
Loose teeth
Teeth that loosen or fall out unexpectedly due to tumor invasion of the bone
Nasal discharge
Discharge from one or both nostrils if the tumor has grown into nasal structures
Weight loss
Loss of appetite and subsequent weight loss as eating becomes uncomfortable
Diagnosis
Your veterinarian will begin with a thorough physical examination, including a careful inspection of the oral cavity. Diagnosis typically involves a combination of the following steps:
Biopsy: A tissue sample is taken from the mass and examined under a microscope. This is the definitive way to confirm a melanoma diagnosis and assess how aggressive the cells appear.
Imaging: Dental X rays, CT scans, or MRI scans may be used to evaluate how deeply the tumor has invaded the jawbone or surrounding structures.
Lymph node evaluation: The regional lymph nodes (often under the jaw) are assessed for enlargement and may be sampled to check for cancer spread.
Chest X rays or CT: To look for evidence of spread to the lungs, which is a common site of metastasis for oral melanoma.
Treatment Options
Treatment for oral melanoma depends on the size and location of the tumor, how deeply it has invaded surrounding tissue, whether it has spread, and the overall health of the dog. Options often used individually or in combination include:
Surgery
Surgical removal is typically the first treatment pursued when feasible. Because oral melanomas frequently invade the underlying bone, surgery may involve removing a portion of the jawbone (mandibulectomy or maxillectomy). While this sounds drastic, most dogs adapt remarkably well after these procedures, maintaining a good quality of life and the ability to eat normally.
Radiation Therapy
Oral melanomas are considered relatively responsive to radiation therapy, particularly for local control of the tumor. Radiation may be used after surgery to reduce the risk of local recurrence, or as the primary treatment when surgery is not possible. It is especially useful for tumors located in difficult areas such as near the back of the mouth.
Immunotherapy and the Melanoma Vaccine
A significant development in the treatment of canine oral melanoma is the availability of a licensed DNA vaccine specifically designed for dogs. This vaccine, produced by Merial (now part of Boehringer Ingelheim) and known as the USDA conditionally approved Oncept canine melanoma vaccine, works by stimulating the immune system to recognize and attack melanoma cells. It is typically administered following surgery or radiation as maintenance therapy. While not a cure, the vaccine has been shown in studies to extend survival times in some dogs with stage II or III oral melanoma.
Chemotherapy
Chemotherapy is generally considered less effective against melanoma than against some other cancers, but it may be used in certain cases, particularly when the disease has spread beyond the local area. It is often considered as a palliative option to slow progression and improve comfort.
Important Note on Prognosis Oral melanoma prognosis depends heavily on the stage at diagnosis. Tumors smaller than 2 cm that have not spread carry a better prognosis than larger, invasive, or metastatic tumors. On average, with surgery alone, median survival times range from 17 to 19 months for stage I disease. The melanoma vaccine combined with surgery or radiation may extend survival times further. However, because oral melanoma is aggressive, it is essential to begin treatment promptly after diagnosis.
Digital Melanoma
Overview
Digital melanoma refers to melanoma that develops on the toes, paws, or nail beds. While melanoma of the digits is less common than oral melanoma, it remains a significant concern because it tends to be highly malignant and has a strong tendency to spread to the lymph nodes and lungs. It is the most common malignant tumor of the canine digit.
Because of its location, digital melanoma can easily be mistaken for a nail infection, a broken nail, or an abscess, leading to delayed diagnosis. Any swelling, mass, or ulceration involving a toe or nail bed that does not resolve with standard treatment should be evaluated further.
Who Is at Risk?
Digital melanoma is more often seen in older large breed dogs. There is a well established breed predisposition in dogs with darkly pigmented skin and coats, including:
Black Labrador Retrievers
Standard Poodles
Schnauzers
Gordon Setters
Giant Schnauzers
The fact that breed and coat color appear to play a role suggests a genetic component to digital melanoma, though the specific mechanisms are still being studied.
Signs and Symptoms
Digital melanoma often causes localized but noticeable changes to the affected toe. Signs to watch for include:
Swelling of one or more toes, often involving the nail bed or the area just behind the nail
Lameness or limping that seems to originate from a specific paw
A mass or lump on the toe, which may be pigmented or unpigmented
Loss of a nail, or a nail that appears to be lifting away from the tissue below
Ulceration or a wound on the toe that does not heal
Bleeding from the toe
Enlargement of the lymph nodes in the area, such as the popliteal node behind the knee
Diagnosis
Diagnosis of digital melanoma begins with a thorough physical examination of the affected paw, followed by additional workup to stage the disease. Diagnostic steps typically include:
Fine needle aspirate or biopsy: Cells or tissue from the mass are examined microscopically. Occasionally the entire digit needs to be removed and submitted for pathology.
X rays of the digit: To determine whether the tumor has invaded the underlying bone (third phalanx), which significantly affects prognosis.
Lymph node assessment: Palpation and possible sampling of the regional lymph nodes to check for spread.
Thoracic imaging: Chest X rays or CT scanning to evaluate the lungs for metastatic disease.
Treatment Options
Amputation of the Digit
The standard surgical treatment for digital melanoma is amputation of the affected toe. This is typically well tolerated by dogs, the majority of whom adapt quickly and maintain good function and quality of life. Wide surgical margins are important to reduce the risk of local recurrence.
Lymph Node Surgery
If regional lymph nodes are confirmed to contain cancer cells, surgical removal of those nodes (lymphadenectomy) may be recommended to reduce the local tumor burden.
Radiation and Immunotherapy
As with oral melanoma, radiation therapy may be used to address residual disease after surgery or to treat cases where complete surgical removal is not possible. The USDA approved canine melanoma vaccine may also be considered as an adjunct therapy, particularly for cases with a higher risk of metastasis.
Prognosis for Digital Melanoma Digital melanoma carries a guarded to poor prognosis, particularly when bone invasion is present at the time of diagnosis. Studies have shown that bone involvement at the time of surgery is associated with shorter survival times. Without bone invasion, some dogs can achieve longer survival times following digit amputation. Thoracic metastasis is unfortunately common, occurring in a significant proportion of affected dogs, which underscores the importance of prompt diagnosis and treatment.
Ocular Melanoma
Overview
Ocular melanoma refers to melanoma involving the eye and its surrounding structures. In dogs, ocular melanoma can develop in several different locations within and around the eye, each with distinct characteristics and implications. The primary forms include uveal melanoma (arising from the uvea, the pigmented middle layer of the eye), limbal or epibulbar melanoma (arising at the junction of the cornea and sclera), and eyelid melanoma.
Ocular melanomas tend to behave less aggressively than oral or digital melanomas in dogs, and many are considered benign or of low malignant potential. However, because they can progressively damage the eye and, in some cases, eventually spread systemically, they still require careful monitoring and management.
Types of Ocular Melanoma in Dogs
Uveal Melanoma
Uveal melanomas arise from the iris, ciliary body, or choroid (the collective structures forming the uvea). They are the most commonly seen intraocular tumors in dogs. These tumors typically appear as dark pigmented lesions on the iris or as a visible discoloration or mass within the eye. While many uveal melanomas in dogs grow slowly and remain locally contained for extended periods, some can become invasive, leading to secondary complications including glaucoma (increased intraocular pressure), lens luxation, hemorrhage, and eventually loss of vision or the eye itself. A small percentage will metastasize.
Limbal or Epibulbar Melanoma
Limbal melanomas arise at the limbus, the border region between the transparent cornea and the white sclera. They typically appear as a raised, dark, well defined mass on the surface of the eye. In dogs, limbal melanomas tend to be relatively benign, growing slowly over months to years. They are more common in large breed dogs and are frequently seen in German Shepherd Dogs, Labrador Retrievers, and Golden Retrievers. Despite their generally benign behavior, they can cause discomfort and corneal irritation if allowed to grow unchecked, and complete removal is usually recommended.
Eyelid Melanoma
Melanoma can also occur on the eyelids. Eyelid tumors in dogs are common overall, and while most are benign, melanoma does occur. Eyelid melanomas can appear as darkly pigmented, raised masses on the margin or surface of the eyelid. They have the potential to invade locally and, less commonly, to spread to other sites. Surgical removal is typically recommended to prevent further local growth and irritation to the eye surface.
Signs and Symptoms
The signs of ocular melanoma vary depending on the location and the degree of growth. Pet owners may notice:
Category
Details
Dark discoloration
A new or growing dark spot on the iris (colored part of the eye) or visible within the eye
Mass on the eye
A raised, pigmented growth at the limbus or on the eyelid margin
Eye redness
Persistent redness or irritation of the eye, often due to secondary inflammation or glaucoma
Eye discharge
Increased tearing or discharge from the affected eye
Cloudiness
A hazy or cloudy appearance to the cornea, sometimes caused by secondary glaucoma
Vision changes
Bumping into objects, reluctance to navigate in dim light, or other signs of reduced vision
Enlarged eye
A visibly larger eye (buphthalmos), indicating elevated intraocular pressure
Squinting
Holding the eye partially or fully closed, suggesting pain or discomfort
Diagnosis
A veterinary ophthalmologist is the ideal specialist to evaluate possible ocular melanoma. Diagnostic evaluation typically includes:
Ophthalmic examination: Using a slit lamp and indirect ophthalmoscopy to examine the structures of the eye in detail, assess the size and extent of any mass, and evaluate intraocular pressure.
Ocular ultrasound: High frequency ultrasound can be used to image the interior of the eye and characterize a mass that may not be fully visible externally.
Histopathology: In most cases, a definitive diagnosis requires tissue sampling. For limbal and eyelid tumors this is generally straightforward. For intraocular tumors, biopsy carries risks, and the decision to pursue it versus proceeding to surgical management is made on a case by case basis.
Systemic staging: While ocular melanomas are less likely to metastasize than oral or digital forms, staging with imaging of the chest and abdomen may be recommended, particularly if the tumor appears aggressive or there are other concerns.
Treatment Options
Observation
For small, slowly growing uveal melanomas that are not causing secondary complications such as glaucoma or discomfort, a period of careful observation with regular monitoring appointments may be the initial approach. This allows the veterinarian to track the growth rate and behavior of the tumor before committing to intervention.
Laser Therapy
Diode laser photocoagulation is sometimes used to treat small uveal melanomas. The laser targets the pigmented tumor cells, with the goal of reducing the tumor and preventing further growth. This approach can be effective for smaller lesions and carries fewer risks than more invasive procedures.
Surgical Excision
For limbal and eyelid melanomas, surgical removal is typically the treatment of choice and often results in excellent outcomes when complete excision is achieved. Cryotherapy (freezing) is sometimes used in combination with or instead of surgery for superficial lesions.
Enucleation
When a uveal melanoma has caused severe intraocular complications, loss of vision, or unmanageable pain, removal of the entire eye (enucleation) may be recommended. While this is a significant decision, most dogs adjust well following the procedure and maintain a good quality of life with one eye. This option also eliminates the tumor and any associated secondary issues such as chronic pain from elevated intraocular pressure.
Prognosis for Ocular Melanoma The prognosis for dogs with ocular melanoma is generally more favorable than for oral or digital melanoma, particularly for limbal and eyelid tumors. Uveal melanomas vary widely in behavior; some remain stable for years while others progress more rapidly. Metastatic rates for canine uveal melanoma are estimated at 4 to 7 percent overall. Regular monitoring is key to catching any changes early and adjusting the management plan accordingly.
Living with a Dog with Melanoma
Supportive Care and Quality of Life
A diagnosis of melanoma in your dog can be frightening and overwhelming. It is important to remember that many dogs continue to live comfortably and happily during and after treatment, and the goal of veterinary oncology is always to maximize both length and quality of life.
Some practical ways to support your dog through treatment and beyond:
Nutritional support: Dogs undergoing treatment may experience changes in appetite. Feeding small, frequent meals of highly palatable, easily digestible food can help maintain body condition. Discuss any supplements or dietary changes with your veterinarian.
Pain management: Effective pain control is a cornerstone of compassionate cancer care. Your veterinary team can recommend appropriate medications to keep your dog comfortable throughout treatment. Non-steroidal anti-inflammatory pain medicines (carprofen, meloxicam, deracoxib, etc.) are often use and combined with other pain medicine such as gabapentin.
Monitoring at home: Regularly check the site of any surgery or the area of concern. Report new swelling, discharge, changes in appetite or behavior, or any other concerns to your veterinarian promptly.
Emotional wellbeing: Dogs are sensitive to their owners’ emotions. Maintaining routines, gentle exercise, and plenty of affection can support your dog’s mental wellbeing during treatment.
Follow up appointments: Adhering to the recommended schedule for rechecks, imaging, and any ongoing therapies such as vaccine booster doses is essential for the best possible outcome.
When to Seek Urgent Veterinary Care
Contact your veterinarian promptly or seek emergency care if your dog experiences any of the following:
Sudden inability to eat, drink, or open the mouth
Rapid or significant swelling of the face, jaw, or affected limb
Uncontrolled bleeding from the mouth, toe, or eye
Sudden severe lameness or inability to bear weight
Acute eye pain, marked squinting, or a sudden change in eye appearance
Labored breathing or persistent coughing, which could suggest lung involvement
Sudden collapse, extreme lethargy, or significant behavioral change
Questions to Ask Your Veterinarian
Being well prepared for appointments with your veterinarian or veterinary oncologist can help you make informed decisions about your dog’s care. Consider asking:
What stage is the tumor, and what does that mean for prognosis?
What are all of the treatment options available, including their benefits and risks?
What is the goal of treatment: cure, long term control, or palliative care?
What signs at home should prompt me to call or bring my dog in urgently?
Is referral to a veterinary oncologist or specialist recommended?
Are there clinical trials or newer therapies that might be appropriate for my dog?
How will treatment affect my dog’s daily life, activity level, and comfort?
What is the estimated cost of the proposed treatment plan?
How often will rechecks or imaging be needed going forward?
A Final Word
A melanoma diagnosis is never easy news to receive, but it is important to know that advances in veterinary medicine have made meaningful treatment possible for many dogs. The availability of the canine melanoma vaccine, improved surgical techniques, and a growing understanding of this disease are giving more dogs more time with the families they love.
Your role as a caring and attentive pet owner is invaluable. Knowing your dog’s normal, conducting regular gentle examinations of the mouth, feet, and eyes, and maintaining a consistent veterinary care schedule are among the most powerful tools available for early detection. When caught early and treated appropriately, many dogs with melanoma go on to live comfortable and fulfilling lives.
Work closely with your veterinary team, ask questions, and advocate for your dog. You are your dog’s most important ally.
This article is intended for general informational purposes only and does not constitute veterinary medical advice. Always consult a licensed veterinarian for diagnosis and treatment of any health concern in your pet.
Understanding Bone Cancer: A Comprehensive Guide for Pet Owners
A cancer diagnosis is one of the most difficult things a pet owner can face. When that diagnosis is osteosarcoma — bone cancer — it can feel especially overwhelming, because osteosarcoma is aggressive, painful, and often strikes beloved pets in what should be the prime of their lives. But knowledge is power, and understanding this disease will help you ask the right questions, make informed decisions, and advocate for your companion with confidence.
This guide covers everything a pet owner needs to know about osteosarcoma in both dogs and cats: what it is, why it happens, how it behaves differently between species, how it is diagnosed and treated, and how to support your pet through every stage.
What Is Osteosarcoma?
Osteosarcoma (OSA) is a malignant tumor that arises from osteoblasts, the cells responsible for building bone. It is the most common primary bone tumor in both dogs and cats, meaning it originates within the bone itself rather than spreading there from another site.
Osteosarcoma is characterized by two features that make it particularly serious. First, it is locally destructive: it invades and destroys the surrounding bone, causing intense pain and weakening the bone to the point where it can fracture spontaneously (a pathologic fracture) even without trauma. Second, it is highly metastatic: it spreads to other parts of the body — most often the lungs — with alarming speed, even before the primary tumor has been detected.
These two features together make osteosarcoma one of the most challenging cancers in veterinary medicine, and understanding them is fundamental to understanding treatment goals and prognosis.
Osteosarcoma in Dogs
How Common Is It?
Osteosarcoma is far more common in dogs than in any other domestic animal. It is estimated that more than 10,000 dogs are diagnosed with osteosarcoma in the United States each year, making it a significant public health concern in the canine population. It accounts for approximately 85–95% of all primary bone tumors diagnosed in dogs.
Which Dogs Are Most at Risk?
Any dog can develop osteosarcoma, but several factors significantly increase the risk:
Size and weight: Osteosarcoma is predominantly a disease of large and giant breeds. Dogs weighing over 40 kg (88 lbs) are at dramatically elevated risk. The heavier the dog, the greater the risk — likely because larger bones experience more mechanical stress over a lifetime.
Age: Most dogs are diagnosed between 7 and 10 years of age, though it can occur in younger dogs, particularly in giant breeds.
Breed: Great Danes, Irish Wolfhounds, Saint Bernards, Rottweilers, Greyhounds, Golden Retrievers, Labrador Retrievers, Doberman Pinschers, and German Shepherds are among the highest-risk breeds.
Sex: Male dogs appear to develop osteosarcoma slightly more often than females.
Prior bone injury or implants: Tumors occasionally develop at the site of a previous fracture repair (especially with metal implants), after radiation therapy, or in areas of chronic bone infection (osteomyelitis).
Where Does It Occur?
In dogs, osteosarcoma has a strong predilection for the long bones of the limbs — particularly around major joints. The classic teaching phrase is “away from the elbow, toward the knee,” reflecting the most common locations:
Distal radius (just above the wrist) — the single most common site in dogs
Proximal humerus (top of the upper arm, near the shoulder)
Distal femur (just above the knee)
Proximal tibia (just below the knee)
Osteosarcoma can also arise in flat bones such as the skull, ribs, vertebrae, and pelvis, though these axial locations are less common (approximately 25% of cases). Axial osteosarcoma often carries a different set of challenges and prognosis.
Signs and Symptoms in Dogs
The most common early sign is lameness — limping that may seem to come on gradually or suddenly. Owners frequently notice:
Progressive lameness on one limb, often initially intermittent
Swelling or a firm mass over a bone or joint
Pain on palpation of the affected area
Reluctance to bear weight, jump, climb stairs, or exercise
Muscle wasting in the affected limb from disuse
In advanced cases, sudden severe lameness or collapse due to a pathologic fracture
Because lameness in large dogs is often attributed to arthritis or joint problems, osteosarcoma can be mistaken for other conditions early in the disease course. Any dog with persistent or unexplained lameness — particularly a large or giant breed — should have X-rays taken promptly.
⚠ Pathologic Fracture — A Medical Emergency If your dog suddenly cannot bear any weight on a limb, cries out in pain, or the limb appears deformed or abnormally angled, seek emergency veterinary care immediately. Pathologic fractures through osteosarcoma lesions are extremely painful and require urgent pain management and stabilization.
Metastatic Behavior in Dogs
One of the most sobering facts about canine osteosarcoma is its early and aggressive metastatic spread. Studies have shown that at the time of diagnosis, an estimated 90–95% of dogs already have microscopic metastatic disease — even though only about 15% have detectable metastases on chest X-rays at presentation. The lungs are the most common site of spread, followed by other bones and soft tissues.
This is why treatment of osteosarcoma in dogs almost always must address not just the local tumor, but the systemic disease as well.
Osteosarcoma in Cats
How Common Is It?
Osteosarcoma is significantly less common in cats than in dogs, representing a much smaller proportion of feline cancers overall. However, when it does occur, it still carries serious implications and requires prompt attention.
Which Cats Are Most at Risk?
Unlike dogs, feline osteosarcoma does not show strong breed predispositions. Key risk factors include:
Age: Most cats are diagnosed at 8 to 10 years of age, though it can occur across a wide age range.
Sex: Male cats may be slightly overrepresented.
Prior injury: As in dogs, osteosarcoma has occasionally been reported at sites of previous trauma, fracture repair, or chronic inflammation in cats.
Where Does It Occur in Cats?
The distribution of osteosarcoma in cats differs notably from dogs. While appendicular (limb) osteosarcoma does occur in cats, a higher proportion of feline cases arise in the axial skeleton — including the skull, mandible (jaw), scapula, pelvis, and vertebrae — compared to dogs.
When feline osteosarcoma does affect the limbs, the hind limbs are more commonly involved than the front limbs, and the tumor tends to occur more distally (lower on the limb) than in dogs.
Signs and Symptoms in Cats
Cats present with signs that depend heavily on the location of the tumor:
Appendicular tumors: Lameness, swelling, or a firm mass over a limb bone
Jaw or skull tumors: Facial swelling, difficulty eating, drooling, or visible mass around the head
Axial tumors: Pain, reluctance to move, or neurological signs (weakness, incoordination) if the spine is affected
General signs: Weight loss, lethargy, and reduced appetite are common across all locations
Key Differences: Dogs vs. Cats
Feature
Dogs vs. Cats
Incidence
Very common in dogs; uncommon in cats
Tumor location
Dogs: predominantly limbs (distal radius most common). Cats: more axial involvement
Breed predisposition
Dogs: large/giant breeds strongly predisposed. Cats: no clear breed link
Dogs: poor (~4 months). Cats: better (~24-28 months with amputation)
Response to chemo
Dogs: well-established protocols. Cats: less data available
Diagnosis
Diagnosing osteosarcoma accurately is essential before any treatment decisions are made. A full diagnostic workup typically includes:
Radiographs (X-Rays)
Plain X-rays of the affected bone are usually the first and most accessible diagnostic step. Osteosarcoma has characteristic radiographic appearances: a mix of bone destruction (lytic areas) and abnormal new bone production (proliferative changes), often described as a “sunburst” pattern. There may also be lifting of the periosteum (the outer bone covering), creating what radiologists call a Codman triangle.
While strongly suggestive, X-ray findings alone cannot confirm osteosarcoma — a tissue sample is required for definitive diagnosis.
Biopsy and Histopathology
A biopsy — removal of a small sample of the tumor — is the only way to definitively confirm osteosarcoma and distinguish it from other bone tumors or infections. This is critically important, as treatment for osteosarcoma differs significantly from treatment for other conditions that can look similar on X-rays (such as fungal infections or other bone tumors). A Jamshidi needle biopsy or incisional biopsy may be performed, often under sedation or anesthesia.
Staging: Assessing the Extent of Disease
Once osteosarcoma is confirmed (or strongly suspected), staging tests help determine how far the disease has spread and guide treatment planning:
Thoracic imaging: Chest X-rays or CT scan of the chest to look for pulmonary metastases (lung spread)
Abdominal ultrasound: Ultrasound of the abdomen to evaluate internal organs for spread
Bloodwork: A complete blood count, chemistry panel, and urinalysis to assess overall organ function and anesthesia risk
Bone scan: A bone scan (nuclear scintigraphy) or whole-body CT can detect spread to other bones, which may not be visible on plain X-rays
Serum alkaline phosphatase: Some specialists measure alkaline phosphatase (ALP) levels, as elevated ALP has been associated with a worse prognosis in dogs with osteosarcoma
Treatment Options
Treatment of osteosarcoma is complex and depends on the location and extent of the tumor, the species and overall health of the patient, and the goals and resources of the owner. In most cases, the best outcomes require a multimodal approach — combining more than one treatment type. There is no single right answer, and the conversation with your veterinary team should be open, honest, and centered on your pet’s quality of life.
Surgery
Amputation
For appendicular (limb) osteosarcoma, amputation of the affected limb is the most effective way to eliminate the local tumor and — critically — to provide immediate and complete relief from the severe bone pain. This is often the single most impactful thing that can be done for an animal’s quality of life.
Many owners are initially reluctant to consider amputation, worried that their pet will not cope on three legs. However, most dogs and cats adapt remarkably well to life as a tripod, often within days to weeks of surgery. Dogs with osteosarcoma are in significant pain before amputation — removing that pain transforms their quality of life almost immediately.
Amputation alone, without chemotherapy, results in a median survival of approximately 4–6 months in dogs (because of rapid metastatic progression). In cats, outcomes after amputation alone are considerably better, with median survival times of approximately 24–28 months, reflecting the less aggressive metastatic behavior of feline osteosarcoma.
Limb-Sparing Surgery
In carefully selected cases — particularly in dogs where amputation is not possible due to pre-existing orthopedic disease in other limbs, or where the owner strongly prefers limb preservation — limb-sparing surgery may be an option. The affected segment of bone is removed and replaced with a bone graft (from a donor or a synthetic implant), with the goal of preserving a functional limb.
Limb-sparing surgery is technically demanding and not universally available. It carries a significant risk of complications, including infection, implant failure, and local tumor recurrence. It is best performed at a veterinary specialty center by an experienced surgical oncologist. Survival times are generally similar to amputation when combined with chemotherapy.
Chemotherapy
Because the vast majority of dogs with osteosarcoma already have microscopic metastatic disease at diagnosis, surgery alone is rarely curative. Chemotherapy is strongly recommended following amputation (or limb-sparing surgery) to target microscopic metastases and significantly prolong survival.
The most commonly used chemotherapy protocols in dogs include:
Carboplatin: A platinum-based drug that damages cancer cell DNA; historically one of the most effective single agents against osteosarcoma
Doxorubicin: Often used in alternating or combination protocols with carboplatin
Gemcitabine: A newer agent increasingly used in combination protocols
With surgery plus chemotherapy, median survival in dogs extends to approximately 10–12 months, with roughly 20–25% of dogs surviving 2 years or more. These numbers represent medians — some dogs do significantly better.
In cats, the use of chemotherapy following surgery is less well-studied, but it is increasingly recommended in cases where complete tumor removal has not been achieved or where spread is suspected.
Radiation Therapy
Radiation therapy plays an important role in several contexts:
Definitive radiation for inoperable tumors: For tumors in locations where surgical removal is not possible (such as the spine, ribs, or skull), stereotactic radiosurgery (SRS) — a highly focused, high-dose radiation technique — can provide meaningful local tumor control.
Palliative radiation for pain relief: For pets whose owners choose not to pursue surgery (or for whom surgery is medically contraindicated), palliative radiation can significantly reduce bone pain and improve quality of life for weeks to months. This does not treat the cancer, but it can make a pet much more comfortable.
Palliative Care (Without Surgery)
For some pets — whether due to advanced disease, other health conditions, financial constraints, or personal preference — aggressive surgical treatment may not be chosen. Palliative care focuses on maximizing comfort and quality of life:
Pain management: NSAIDs (such as meloxicam or carprofen in dogs), opioids, gabapentin, and other agents can significantly reduce bone pain. Pain management is a cornerstone of palliative OSA care.
Bisphosphonate therapy (e.g., pamidronate, zoledronate): Protects weakened bones from fracture and reduces pain during movement in some cases.
Palliative radiation: As described above, can reduce pain and may slow local tumor progression.
Metronomic chemotherapy: Short courses of anti-cancer medications may slow progression while minimizing side effects.
Questions to Ask Your Veterinary Team What type of osteosarcoma does my pet have, and where exactly is it? Has the cancer spread, and if so, where? What treatment options are available for my pet specifically? What is the realistic prognosis with each option? What are the expected side effects and quality-of-life implications? What does palliative care look like if we choose not to pursue surgery? Would a referral to a veterinary oncologist be beneficial? Are there any clinical trials my pet might qualify for?
Pain Management: A Priority at Every Stage
Osteosarcoma is one of the most painful cancers in veterinary medicine. The bone pain it causes is intense and constant, similar to what humans with bone cancer describe. Regardless of which treatment path you choose, aggressive pain control is not optional — it is a fundamental ethical obligation and the most direct way to preserve your pet’s quality of life.
Signs of bone pain in dogs and cats can include:
Reluctance to move, jump, climb stairs, or be active
Crying out, whimpering, or vocalizing
Guarding the affected limb or refusing to bear weight
Changes in behavior: aggression, withdrawal, hiding (particularly in cats), loss of interest in food or interaction
Panting or restlessness at night (a common sign of pain in dogs)
A glazed, distant expression or failure to respond normally
Do not hesitate to contact your veterinarian if you believe your pet’s pain is not adequately controlled. Pain management regimens often need to be adjusted as the disease progresses, and your observations at home are invaluable to your veterinary team.
Prognosis and What to Expect
Dogs
Canine osteosarcoma carries a serious prognosis due to its aggressive metastatic behavior. Without treatment, the prognosis is very poor — most dogs are humanely euthanized within 1–4 months of diagnosis due to uncontrolled pain or disease progression. With palliative care alone, survival is typically 1–4 months. With amputation alone (no chemotherapy), median survival is approximately 4–6 months. With amputation plus chemotherapy, median survival extends to 10–12 months, and approximately 20–25% of dogs survive 2 years or more.
Factors associated with a better prognosis in dogs include: lower serum alkaline phosphatase levels, tumor located in the radius (vs. other sites), no detectable metastasis at diagnosis, and complete surgical removal of the tumor.
Cats
The prognosis for cats with osteosarcoma is generally more favorable than for dogs, primarily because feline osteosarcoma tends to be less aggressively metastatic. After amputation, cats have a reported median survival of approximately 24–28 months, with a significant proportion surviving 3 or more years. This is dramatically better than the canine situation, making aggressive surgical treatment a particularly worthwhile investment in appropriate feline patients.
Axial (non-limb) osteosarcoma in cats, as in dogs, tends to carry a more guarded prognosis due to the difficulty of achieving complete surgical removal.
The Role of a Veterinary Oncologist
Veterinary oncology is a board-certified specialty dedicated to the diagnosis and treatment of cancer in animals. For a disease as complex as osteosarcoma, a referral to a veterinary oncologist can be enormously beneficial:
Oncologists perform and interpret advanced imaging (CT scans, bone scans) that may not be available at a general practice.
They can guide biopsy technique to maximize diagnostic accuracy and minimize complications.
They design and oversee chemotherapy protocols, monitor for side effects, and adjust treatment as needed.
They work closely with veterinary surgeons specializing in surgical oncology for limb-sparing or complex axial procedures.
They can discuss clinical trial options that may give your pet access to cutting-edge treatments.
They provide honest, detailed prognostic information to help you make decisions that align with your values and your pet’s quality of life.
Your primary care veterinarian and the oncology team work together — a referral is not a rejection, but an expansion of your pet’s care team.
Supporting Your Pet Through Osteosarcoma
Caring for a pet with cancer is emotionally and practically demanding. The following can help both you and your pet navigate the journey:
At Home
Medications: Give all prescribed medications on schedule. Consistency in pain management is critical.
Comfortable environment: Provide soft, comfortable, easily accessible resting areas. Orthopedic foam beds can reduce discomfort. Consider ramps instead of stairs.
Gentle exercise: Short, gentle outings rather than long walks. Let your pet set the pace and avoid forced activity. Activity can be beneficial for morale but must be appropriate to the current level of pain.
Nutrition: Maintain good nutrition. If your pet’s appetite changes, ask your vet about appetite stimulants or dietary adjustments.
Monitor closely: Watch for changes in breathing (which may indicate lung metastasis), sudden severe pain (which may indicate fracture), or significant deterioration in mobility or demeanor — and contact your vet promptly.
Emotional Support for Pet Owners
Grief, guilt, and anxiety are entirely normal when facing a pet’s serious illness. You may find yourself struggling with decisions about treatment intensity, cost, and ultimately end-of-life care. There is no universally right answer — only what is right for your pet and your family.
Many veterinary schools and specialty centers offer support resources for pet owners facing serious diagnoses, including social workers, grief counselors, and owner support groups. Do not hesitate to ask your veterinary team for these resources if you are struggling.
End-of-Life Decisions
One of the most profound gifts we can give our animals is freedom from unmanageable suffering. As osteosarcoma progresses, there often comes a time when pain can no longer be adequately controlled, quality of life has declined significantly, and the kindest choice is humane euthanasia. This is not failure — it is the ultimate act of love and advocacy for your companion.
Discussing end-of-life preferences and quality-of-life benchmarks with your veterinary team early in the process can make this deeply difficult decision somewhat clearer when the time comes. Quality-of-life scales (such as the HHHHHMM scale) can be helpful tools for tracking your pet’s wellbeing over time.
Research and Hope for the Future
Osteosarcoma research in veterinary medicine is active and advancing. Because canine osteosarcoma closely resembles human pediatric osteosarcoma in its biology and behavior, dogs with OSA are recognized as a valuable spontaneous model for developing better treatments — research that benefits both species.
Current areas of investigation include:
Targeted therapies and tyrosine kinase inhibitors: Drugs that specifically target molecules driving OSA cell growth and survival
Immunotherapy and cancer vaccines: Treatments that help the immune system recognize and attack osteosarcoma cells
Inhaled and regional chemotherapy: Novel delivery methods that concentrate chemotherapy directly in bone tissue, improving efficacy and reducing systemic side effects
Genomic profiling and precision oncology: Analyzing tumor genetics to identify individual tumors’ specific drivers and predict which treatments will work best for each patient
Clinical trials: Studies recruiting dogs with naturally occurring osteosarcoma to test new treatments, potentially offering your pet access to cutting-edge therapies before they become widely available
Ask your veterinary oncologist whether any clinical trials are currently enrolling patients that your pet might qualify for. Participation in a clinical trial can sometimes provide access to novel therapies at reduced or no cost, while also contributing to knowledge that will help future patients.
Final Thoughts
A diagnosis of osteosarcoma is serious — there is no minimizing that. But it is not the end of the conversation, and it does not define the entirety of your time with your companion. Many dogs and cats with OSA have weeks or months of genuinely good days following diagnosis and treatment. Your job is to make as many of those days as possible as comfortable and meaningful as they can be.
Ask questions. Advocate for your pet. Seek specialist input. Control pain aggressively. And allow yourself the space to grieve, even while your pet is still with you — anticipatory grief is real and valid.
The bond between you and your pet is not measured in the quantity of days, but in the quality of care and love you give each other. In that sense, facing this disease with knowledge and compassion is one of the deepest expressions of that bond.
This article is intended for general educational purposes only and does not constitute veterinary medical advice. Always consult your veterinarian or a board-certified veterinary oncologist for diagnosis and treatment recommendations specific to your pet.
Learning that your cat has lymphoma can be frightening and heartbreaking. Lymphoma is the most common cancer diagnosed in cats, yet it is also one of the most manageable — particularly the form most frequently seen. Understanding the disease, how it is diagnosed, and what treatment options are available will help you make confident, informed decisions alongside your veterinary team.
What Is Lymphoma? Lymphoma is a cancer of lymphocytes, the white blood cells responsible for immune defense. Because lymphocytes circulate throughout the body and reside in lymph nodes, the spleen, the intestines, and many other organs, lymphoma in cats can arise in numerous locations. Unlike some other cancers, feline lymphoma frequently involves the gastrointestinal tract rather than the lymph nodes, which makes it quite different from what is typically seen in dogs.
The Most Common Form: Gastrointestinal Lymphoma
The gastrointestinal (GI) tract is by far the most common site of lymphoma in cats, accounting for approximately 50–75% of all feline lymphoma cases. GI lymphoma is divided into two main subtypes that differ dramatically in behavior, treatment, and outlook.
Small Cell (Low-Grade) Lymphoma
Small cell lymphoma — also called low-grade lymphoma or small cell lymphocytic lymphoma — is the most frequently diagnosed subtype in cats. It primarily affects the small intestine and typically progresses slowly over months to years. Many cats with small cell lymphoma are older, commonly 9–15 years of age, and may have been showing subtle signs for some time before a diagnosis is made.
Small cell lymphoma is considered an indolent or slow-growing cancer. With treatment, the prognosis is genuinely encouraging. Many cats achieve a good quality of life for two years or longer, and some do exceptionally well for three years or more. It is not uncommon for owners to describe their treated cats as “acting like themselves again” within weeks of starting therapy.
An important related condition: small cell lymphoma can be very difficult to distinguish from inflammatory bowel disease (IBD), even under the microscope. Both conditions cause similar intestinal changes, and some researchers believe IBD may progress to lymphoma over time. Your veterinarian may need advanced tissue sampling to tell them apart.
Large Cell (High-Grade) Lymphoma
Large cell lymphoma — also called high-grade or large granular lymphocyte (LGL) lymphoma — is a more aggressive form. It tends to progress rapidly and requires more intensive treatment. Response rates to chemotherapy are lower than for small cell lymphoma, and survival times are typically measured in months rather than years. However, some cats do achieve meaningful remissions with treatment.
Why the Distinction Matters Knowing whether your cat has small cell or large cell GI lymphoma is one of the most important pieces of information your veterinary team needs. The two subtypes require completely different treatment protocols and carry very different prognoses. This distinction cannot be made from a fine needle aspirate alone — it typically requires a biopsy with histopathology and often immunohistochemistry or PARR testing.
Other Forms of Feline Lymphoma
Although GI lymphoma is the most common, cats can develop lymphoma in several other locations.
Mediastinal Lymphoma
This form involves a large mass in the chest cavity, often originating from the thymus. It is strongly associated with feline leukemia virus (FeLV) infection and tends to affect younger cats. Signs include rapid or labored breathing, open-mouth breathing, and reduced exercise tolerance due to fluid accumulation around the lungs. Mediastinal lymphoma often responds well to chemotherapy initially, and some cats achieve prolonged remissions.
Nasal Lymphoma
Nasal lymphoma arises in the nasal passages and is one of the more favorable forms of the disease. Signs include chronic sneezing, nasal discharge (sometimes bloody), facial swelling, and noisy breathing. Radiation therapy is the preferred treatment and can lead to remission lasting a year and a half to two years or longer in many cats.
Renal (Kidney) Lymphoma
The kidneys are a relatively common site for lymphoma in cats. Both kidneys are usually involved, and they may feel enlarged on physical examination. Signs mimic chronic kidney disease: weight loss, increased thirst and urination, decreased appetite, and vomiting. Renal lymphoma carries a more guarded prognosis than GI or nasal forms. Notably, it has a higher risk of spreading to the central nervous system, which may influence treatment decisions.
Spinal and CNS Lymphoma
Lymphoma involving the spinal cord or brain is uncommon but serious. Signs depend on the location of the tumor and can include hindlimb weakness or paralysis, loss of bladder or bowel control, altered behavior, or seizures. Prognosis is generally guarded, though some cats respond temporarily to steroids and chemotherapy.
Peripheral Nodal Lymphoma
Some cats develop lymphoma primarily in the peripheral lymph nodes — similar to the most common presentation in dogs. This form is less common in cats but does occur. Response to chemotherapy varies depending on the cell type and grade.
Clinical Signs
The signs of feline lymphoma depend on which part of the body is affected. Because GI lymphoma is so prevalent, many of the most common signs are digestive in nature.
Gastrointestinal Lymphoma — Common Signs
Weight loss: Often the earliest and most consistent sign, even when appetite seems normal
Vomiting, which may be intermittent or chronic
Diarrhea, which may be soft, watery, or contain blood or mucus
Decreased appetite or selective eating
Increased appetite in some cats (paradoxically, due to poor nutrient absorption)
Lethargy and reduced activity
A thickened or uncomfortable abdomen on palpation
Mediastinal Lymphoma — Common Signs
Rapid, labored, or open-mouth breathing
Reduced tolerance for exercise or activity
Muffled heart sounds or breath sounds
Regurgitation of food
Compression of the windpipe causing wheezing
Nasal Lymphoma — Common Signs
Persistent sneezing
Nasal discharge from one or both nostrils (clear, mucoid, or bloody)
Noisy or difficult breathing through the nose
Facial asymmetry or swelling over the bridge of the nose
Reduced sense of smell leading to appetite loss
Renal Lymphoma — Common Signs
Weight loss and muscle wasting
Increased thirst and urination
Vomiting and reduced appetite
Large, firm kidneys detectable on physical examination
Many of these signs — especially weight loss, vomiting, and appetite changes — are common to a wide variety of feline conditions. This is why a proper diagnosis is so important: lymphoma can mimic hyperthyroidism, inflammatory bowel disease, kidney disease, and other illnesses, and each requires different management.
Diagnosis
Diagnosing feline lymphoma accurately — and determining the specific type — requires a systematic approach. Your veterinarian may recommend several of the following tests.
Physical Examination
A thorough physical exam includes assessment of body weight and condition, palpation of the abdomen for thickened intestinal loops or enlarged organs, evaluation of peripheral lymph nodes, and listening to the chest. Many cats with GI lymphoma have a palpably thickened small intestine.
Blood and Urine Tests
A complete blood count (CBC), biochemistry panel, and urinalysis help assess overall health, identify anemia, elevated kidney values, or electrolyte disturbances, and establish baselines before starting treatment. These tests alone cannot diagnose lymphoma but are an essential part of the workup.
Feline Leukemia Virus (FeLV) and FIV Testing
FeLV is a significant risk factor for certain forms of feline lymphoma, particularly mediastinal lymphoma in young cats. Testing for FeLV and FIV is routinely recommended for any cat with a lymphoma diagnosis.
Abdominal Ultrasound
Ultrasound is one of the most valuable tools for evaluating feline GI lymphoma. It can visualize the layers of the intestinal wall, identify thickened segments, detect enlarged lymph nodes, assess the spleen and liver, and guide needle aspirates or biopsies. An experienced ultrasonographer can often identify characteristic patterns that suggest lymphoma.
Fine Needle Aspirate (FNA)
A fine needle is inserted into a mass, lymph node, or affected organ to collect cells for microscopic examination (cytology). FNA is quick and minimally invasive. It can confirm the presence of lymphoma in some cases — particularly with large cell or nodal disease — but has significant limitations for diagnosing small cell GI lymphoma, because the cells may appear normal or only mildly abnormal.
Endoscopy and Biopsy
Endoscopy involves passing a small camera into the stomach and intestines while the cat is under anesthesia, allowing small biopsy samples to be collected. Endoscopic biopsies are less invasive than surgery but may not sample deeply enough into the intestinal wall to distinguish small cell lymphoma from IBD reliably.
Surgical (Full-Thickness) Biopsy
A surgical biopsy removes a full-thickness section of the intestinal wall, providing a larger and more complete tissue sample. This is considered the gold standard for diagnosing and subtyping GI lymphoma. While it requires general anesthesia and a recovery period, it provides the most definitive information and is often recommended when endoscopic biopsies are inconclusive.
Immunohistochemistry and PARR Testing
These advanced laboratory tests help classify lymphoma as B-cell or T-cell in origin and determine whether a population of lymphocytes is truly cancerous (clonal) or reactive. They are particularly useful when biopsy results are ambiguous — for example, when distinguishing small cell lymphoma from severe IBD. PARR (PCR for antigen receptor rearrangement) can be performed on tissue or fine needle aspirate samples.
Why Biopsy Matters So Much in Cats In feline GI lymphoma, getting the right type of biopsy can make a significant difference in how well the cancer is classified and treated. Small cell lymphoma and inflammatory bowel disease can look virtually identical on cytology and even on superficial biopsies. A full-thickness surgical biopsy combined with immunohistochemistry gives your veterinary team the clearest picture — and the best foundation for a treatment plan.
Treatment Options
Treatment depends on the form and grade of lymphoma, your cat’s overall health, and your goals and circumstances. The good news is that the most common form — small cell GI lymphoma — is treated with oral medications at home and is generally very well tolerated.
Small Cell GI Lymphoma: Oral Chlorambucil and Prednisone
The standard treatment for small cell lymphoma is a combination of two oral medications: chlorambucil (an alkylating chemotherapy agent) and prednisone (a corticosteroid). Both are given by mouth at home, making this one of the most convenient cancer treatments in veterinary medicine. Chlorambucil is typically given every one to two weeks; prednisone is given daily and gradually tapered.
Response rates are excellent. Approximately 70–90% of cats achieve a good response. Many cats show noticeable improvement within two to four weeks: weight gain, improved appetite, more normal stools, and increased energy. Side effects are uncommon and usually mild: occasional gastrointestinal upset or, rarely, bone marrow suppression. Periodic blood monitoring is recommended to catch any issues early.
Large Cell GI Lymphoma: CHOP-Based Chemotherapy
High-grade lymphoma requires more aggressive treatment using a combination chemotherapy protocol similar to what is used for dogs — typically incorporating drugs such as cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP). These treatments are administered by injection in the clinic on a weekly to biweekly schedule. While cats generally tolerate chemotherapy better than humans, side effects such as nausea, low white blood cell counts, and fatigue can occur. Response rates for high-grade disease are lower than for small cell lymphoma, and remissions are typically shorter.
Mediastinal Lymphoma: Chemotherapy
Mediastinal lymphoma often responds well to chemotherapy, particularly protocols using vincristine, cyclophosphamide, and prednisone (COP) or full CHOP. Before chemotherapy can begin, any fluid around the lungs (pleural effusion) is drained to help the cat breathe more comfortably. Some cats achieve remissions lasting six months to over a year.
Nasal Lymphoma: Radiation Therapy
Radiation is the treatment of choice for nasal lymphoma and is associated with some of the longest survival times of any feline lymphoma form. Treatment typically involves a series of radiation sessions at a veterinary radiation oncology facility. Chemotherapy may be added to reduce the risk of systemic spread. Most cats tolerate radiation well, with temporary side effects including nasal irritation and discharge during treatment.
Supportive and Palliative Care
For cats that are too ill for chemotherapy, or whose owners prefer comfort-focused care, prednisone alone can temporarily improve quality of life, reduce inflammation, and stimulate appetite. While not a curative treatment, prednisone can provide weeks to a couple of months of improved wellbeing. Nutritional support, anti-nausea medications, appetite stimulants, and fluid therapy can all play important supportive roles regardless of the primary treatment chosen.
Chemotherapy Tolerability in Cats Cats are often described as the best chemotherapy patients in veterinary medicine. The doses used are calibrated to preserve quality of life, not to push toward cure at all costs. Most cats receiving chemotherapy continue to eat well, groom themselves, and behave normally between treatments. Side effects serious enough to require hospitalization are uncommon. If your cat is not tolerating a protocol well, doses can be adjusted or drugs can be changed — open communication with your veterinary oncologist is key.
Prognosis
Prognosis in feline lymphoma varies considerably by form, grade, and treatment. The table below summarizes general expectations for the most common presentations.
Form of Lymphoma
Treatment
Median Survival
Small cell (low-grade) GI
Chlorambucil + prednisone
2–3+ years
Large cell (high-grade) GI
CHOP chemotherapy
3–9 months
Mediastinal
Chemotherapy (COP/CHOP)
3–12+ months
Nasal
Radiation ± chemotherapy
1.5–2+ years
Renal
Chemotherapy
3–6 months
Spinal/CNS
Chemotherapy ± steroids
Weeks to months
Several factors are associated with a better outcome:
Small cell (low-grade) disease: By far the most favorable subtype — many cats live two years or longer
B-cell immunophenotype: Generally responds better than T-cell or null-cell disease
Good body condition and normal bloodwork at diagnosis: Indicates the cat can tolerate treatment well
Achieving complete remission: Cats that reach a complete response tend to survive longer than those with a partial response
No involvement of the bone marrow or blood: Localized disease generally carries a better prognosis
It is worth noting that even cats with a less favorable prognosis can often enjoy a meaningful quality of life during treatment. Veterinary oncologists focus not just on extending life but on making the time that remains as comfortable and enjoyable as possible for your cat and your family.
Working With Your Veterinary Team
Managing feline lymphoma is a team effort between you, your primary care veterinarian, and often a board-certified veterinary oncologist. Oncologists are specialists who can offer access to the latest protocols, advanced diagnostics, and clinical trials not available at general practices.
Questions to consider asking at your oncology consultation:
What type and grade of lymphoma does my cat have — small cell or large cell?
Is this B-cell or T-cell, and what does that mean for treatment?
What treatment options do you recommend, and what are the expected response rates?
How will treatment be administered — at home or in the clinic?
How often will my cat need monitoring and check-ups?
What side effects should I watch for, and when should I call you?
Is my cat a candidate for any clinical trials?
How will we know if treatment is working?
What signs would suggest my cat is no longer comfortable or benefiting from treatment?
A lymphoma diagnosis changes things — but it does not have to mean the end of a happy life for your cat. Many cats with lymphoma, especially the small cell form, continue to thrive for years after diagnosis, eating well, playing, and enjoying their families. You know your cat better than anyone, and your observations and partnership with your veterinary team are among the most powerful tools in managing this disease.
This document is intended for informational purposes only and does not replace professional veterinary advice, diagnosis, or treatment. Always consult a licensed veterinarian or board-certified veterinary oncologist regarding your cat’s specific condition.
Receiving a lymphoma diagnosis for your dog can be overwhelming. Lymphoma is one of the most common cancers seen in dogs, but it is also one of the most treatable. Understanding what lymphoma is, how it is diagnosed, and what treatment options are available can help you make informed decisions about your dog’s care and feel more confident during this difficult time.
What Is Lymphoma? Lymphoma (also called lymphosarcoma) is a cancer that arises from lymphocytes — a type of white blood cell that is part of the immune system. Because lymphocytes are found throughout the body in lymph nodes, the spleen, bone marrow, blood, and other organs, lymphoma can occur almost anywhere. It is not a single disease but rather a group of related cancers that vary in location, behavior, and outlook.
Forms of Lymphoma in Dogs
Dogs can develop lymphoma in several different locations in the body, each with its own characteristics.
Multicentric Lymphoma
This is by far the most common form, accounting for roughly 80–85% of all canine lymphoma cases. It affects multiple lymph nodes throughout the body simultaneously — you may notice swollen lumps under the jaw, in front of the shoulders, behind the knees, or in the groin. Affected dogs often appear relatively well early in the disease despite dramatic lymph node enlargement.
Alimentary (Gastrointestinal) Lymphoma
This form targets the gastrointestinal tract, including the stomach, small intestine, large intestine, and sometimes the liver or spleen. Signs center on digestive upset: vomiting, diarrhea, weight loss, and loss of appetite. It is the second most common form and can be more challenging to diagnose and treat.
Mediastinal Lymphoma
Mediastinal lymphoma involves the lymph nodes or thymus located in the chest (mediastinum). The accumulation of a large mass and/or fluid in the chest cavity puts pressure on the lungs and heart, causing breathing difficulties. This form is sometimes associated with a condition called hypercalcemia (elevated blood calcium), which can cause additional symptoms.
Cutaneous (Skin) Lymphoma
This rarer form originates in the skin. It may appear as single or multiple patches, plaques, nodules, or ulcerated sores anywhere on the body, including the mouth. Cutaneous lymphoma can look like many other skin conditions, which can delay diagnosis. It is divided into subtypes (epitheliotropic and non-epitheliotropic) that behave quite differently from one another.
Extranodal Lymphoma
Lymphoma can also arise in virtually any other organ — the eyes, central nervous system, kidneys, nasal passages, or bone marrow. These forms are uncommon but tend to present with signs related to the specific organ involved (e.g., seizures with brain involvement, or nosebleeds with nasal lymphoma).
B-Cell vs. T-Cell Lymphoma Lymphocytes come in two main types — B cells and T cells — and lymphoma can arise from either. B-cell lymphoma is more common (roughly 60–70% of cases) and generally responds better to treatment. T-cell lymphoma tends to be more aggressive and carries a less favorable prognosis. Your veterinarian can determine which type your dog has through specialized testing, which is important for treatment planning.
Clinical Signs
The signs of lymphoma vary depending on which form is present, but there are some common patterns to watch for.
Multicentric Lymphoma — Common Signs
Painless, firm, rubbery swelling of the lymph nodes (under the jaw, in front of the shoulders, behind the knees, or in the groin)
Lethargy and decreased energy
Reduced appetite or weight loss
Increased thirst and urination (especially if hypercalcemia is present)
Weakness or exercise intolerance
Alimentary Lymphoma — Common Signs
Chronic or intermittent vomiting
Diarrhea, which may contain blood
Progressive weight loss and muscle wasting
Decreased appetite
Abdominal discomfort or a palpable mass in the belly
Mediastinal Lymphoma — Common Signs
Labored or rapid breathing
Exercise intolerance or sudden collapse
Regurgitation of food
Swelling of the face or front limbs (due to reduced blood return)
Increased thirst and urination if hypercalcemia is present
Cutaneous Lymphoma — Common Signs
Itchy, flaky, or reddened skin patches
Raised plaques, nodules, or ulcerated sores
Lesions inside the mouth, causing drooling or difficulty eating
Hair loss in affected areas
If your dog has any of these signs — particularly unexplained lumps, weight loss, or breathing changes — it is important to see your veterinarian promptly. Early detection generally improves outcomes.
Diagnosis
Diagnosing lymphoma typically involves a combination of physical examination, laboratory testing, and tissue sampling. Your veterinarian may perform several of the following:
Physical Examination
A thorough physical exam is the starting point. Your vet will check all accessible lymph nodes for swelling and assess the abdomen for organ enlargement or masses.
Fine Needle Aspirate (FNA)
This quick, minimally invasive procedure involves inserting a small needle into an enlarged lymph node or mass to collect cells for examination under a microscope (cytology). It is often the first step toward a diagnosis and can frequently confirm lymphoma without requiring surgery.
Biopsy
A tissue biopsy — removing a small piece of a lymph node or mass — provides more detailed information than an FNA alone. It allows pathologists to classify the specific type of lymphoma and identify whether it is high-grade or low-grade (indolent), which significantly affects treatment choices and prognosis.
Immunophenotyping
This specialized test determines whether the lymphoma is B-cell or T-cell in origin. It can be performed on FNA samples or biopsy tissue and is an important part of treatment planning, since B-cell and T-cell lymphomas respond differently to chemotherapy.
Blood and Urine Tests
A complete blood count (CBC), biochemistry panel, and urinalysis help assess your dog’s overall health, identify abnormalities such as elevated calcium or anemia, and establish baseline values before starting treatment.
Imaging
Chest X-rays and abdominal ultrasound are used to evaluate the extent of disease — known as staging — and to look for involvement of internal organs. Staging helps your veterinarian tailor the treatment plan and give you a realistic expectation of outcomes.
Understanding Cancer Staging Lymphoma in dogs is staged from I to V based on how widespread the disease is. Stage I is the most localized (a single lymph node), while Stage V indicates involvement of the blood or bone marrow. Higher stages are associated with a more guarded prognosis, though many dogs in advanced stages still respond well to treatment.
Treatment Options
The goal of treatment is to achieve remission — a state in which the cancer is no longer detectable — and to maintain a good quality of life for as long as possible. There is no one-size-fits-all approach; the best option depends on the type and stage of lymphoma, your dog’s overall health, and your own circumstances.
Combination Chemotherapy (CHOP Protocol)
For multicentric B-cell lymphoma, the CHOP protocol is considered the gold standard. CHOP stands for the four drugs used: cyclophosphamide, doxorubicin, vincristine, and prednisone. Treatments are given over approximately 19–25 weeks, with visits typically weekly at first and then spread out. This protocol achieves remission in roughly 80–90% of eligible dogs, with a median survival time of 12–14 months. Approximately 20–25% of dogs live two years or longer.
Single-Agent Chemotherapy
For owners who prefer a simpler schedule or whose dogs cannot tolerate the full CHOP protocol, single-agent options such as doxorubicin alone, chlorambucil, or lomustine (CCNU) may be considered. These tend to produce shorter remission times but can still provide meaningful quality time.
Prednisone (Steroid) Alone
Prednisone, a corticosteroid, can temporarily shrink lymph nodes and improve a dog’s well-being without the rigors of chemotherapy. It is not a curative option — median survival on prednisone alone is typically one to two months — but it may be the most appropriate choice when chemotherapy is not possible. One important caveat: prior treatment with prednisone can reduce the subsequent response to chemotherapy, so this decision should be discussed carefully with your vet.
Targeted Therapies
Newer targeted drugs, such as rabacfosadine (Tanovea) for certain T-cell lymphomas, offer additional options, particularly for cases that do not respond to or have relapsed after CHOP. Your oncologist can advise whether targeted agents are appropriate for your dog’s specific diagnosis.
Radiation Therapy
Radiation is not a primary treatment for systemic lymphoma but may be used for localized forms — such as cutaneous or nasal lymphoma — or as palliative therapy to reduce a mass causing pain or obstruction.
Tolerability of Chemotherapy in Dogs
Many owners are understandably concerned about chemotherapy side effects. Dogs generally tolerate chemotherapy much better than humans, because the doses used are calculated to maximize quality of life rather than to cure. Roughly 75–80% of dogs experience few or no significant side effects. When side effects do occur — such as mild nausea, reduced appetite, or a temporary dip in white blood cell counts — they are usually manageable with supportive medications and resolve quickly.
Quality of Life Is the Priority Veterinary oncologists are committed to keeping your dog comfortable and happy during treatment. If your dog is not feeling well on a particular protocol, doses can be adjusted or drugs can be substituted. Open communication with your veterinary team is essential — always let them know if you notice any changes in your dog’s appetite, energy, or behavior.
Prognosis
Prognosis varies widely depending on the form of lymphoma, the cell type (B-cell vs. T-cell), the stage of disease, and the treatment chosen. The table below summarizes general expectations:
Form of Lymphoma
Treatment
Median Survival
Multicentric (high-grade)
CHOP chemotherapy
12–14 months
Multicentric (high-grade)
Single-agent prednisone only
1–2 months
Alimentary
Chemotherapy (variable)
2–12 months
Mediastinal
Chemotherapy
Months to > 1 year
Cutaneous
Varies by subtype
Months to years
Indolent/low-grade
Chemotherapy or watchful waiting
1–3+ years
Several factors are associated with a better prognosis:
B-cell rather than T-cell immunophenotype
High-grade lymphoma that is chemotherapy-naive (never previously treated)
Good overall health and normal calcium levels at diagnosis
Achieving a complete remission (all detectable cancer disappears) rather than a partial remission
It is also important to understand the concept of rescue chemotherapy. If lymphoma relapses after an initial remission, additional protocols can sometimes induce a second remission. These tend to be shorter and less durable, but they can add quality time for many dogs.
Choosing the Right Path for Your Family There is no wrong decision when it comes to treating your dog’s lymphoma. Some families choose aggressive treatment with the goal of maximum survival time; others prioritize minimizing veterinary visits and keeping daily life as normal as possible. Both are valid, loving choices. Palliative care focused on comfort and quality of life is always an option and can be deeply meaningful. Discuss your goals honestly with your veterinary team so they can recommend the approach that is right for you and your dog.
Working With Your Veterinary Team
Lymphoma is typically managed by a team that may include your primary care veterinarian and a board-certified veterinary oncologist. Oncologists have specialized training in cancer diagnosis and treatment and can offer access to the most current protocols and clinical trials.
Questions worth asking at your first oncology appointment:
What type and stage of lymphoma does my dog have?
Is this B-cell or T-cell lymphoma, and how does that affect the prognosis?
What treatment options do you recommend, and why?
What is the expected response rate and survival time with each option?
How often will my dog need to come in for treatment?
What side effects should I watch for at home?
Are there any clinical trials my dog might be eligible for?
What signs would indicate that my dog is no longer comfortable with treatment?
A lymphoma diagnosis is life-changing, but you do not have to face it alone. With the right support, many dogs with lymphoma continue to enjoy a high quality of life — going for walks, playing, eating well, and spending precious time with their families. Your veterinary team is your partner throughout this journey.
This document is intended for informational purposes only and does not replace professional veterinary advice, diagnosis, or treatment. Always consult a licensed veterinarian or board-certified veterinary oncologist regarding your dog’s specific condition.